Introduction
Introduction
The skin is the most superficial part of the body. The signs of ageing are most visible in the skin. Although, ageing skin is not a threat to a person, it can have a detrimental effect on the psychology of a person. A look into the causes of skin ageing, the available treatments and preventive measures for this inevitable change is important to help both the already aged, as well as, the youth.
This is a 4 part article in which:
- Part 1 – Discusses the structure of skin and its different components
- Part 2 – Discusses cutaneous ageing and its causes
- Part 3 – Discusses the characteristics of ageing skin and the changes in skin appearance
- Part 4 – Discusses products and treatments for skin ageing
a) Sunscreen Agents
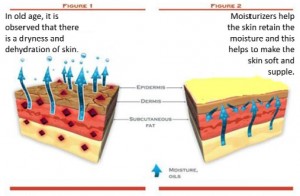
b) Moisturizers
c) Antioxidants
d) Make Up
e) Dermal Fillers
f) Chemical Peels
g) Botulinum Toxin
h) Estrogen and Hormonal Treatments (current article)
i) Plastic Surgery
Estrogens1,2
Skin ageing process increases rapidly after age of 50, especially in women. Skin ageing is influenced by genetic, environmental and hormonal factors. Estrogen affects several skin functions such as, elasticity, water holding capacity, pigmentation and vascularity. It prevents skin ageing by influencing skin thickness, skin wrinkling and skin moisture.
EFFECTS OF ESTROGEN
a) Estrogen Effect on Skin Thickness and Collagen Content
Postmenopausal women with osteoporosis had skin that was atrophied with decreased skin thickness, skin collagen content and reduction in bone marrow density. It was observed that there was decreased in Type I and Type III collagen as well as, decrease in type III/type I ratio in comparison to premenopausal women. Skin collagen decline was closely related to the number of years following menopause. With the correlation noted between skin collagen decline and postmenopausal years, studies have attempted to decipher the effects of estrogens on skin collagen. Several studies have shown that estrogen therapy has had beneficial effects on collagen content and skin thickness.
b) Estrogen Effects on Skin Moisture
Ability of skin to hold water is by two mechanisms
- Using Stratum Corneum Lipids
- Using Dermal Glycosaminoglycans.
Postmenopausal women not taking estrogen experienced dry skin compared to those with estrogen therapy. Transdermal estrogen therapy leads to an increased water holding capacity of stratum corneum. Estrogen therapy has shown to increase dermal water holding capacity in animals and increase in glycosaminoglycans within 2 weeks of estrogen therapy, while in humans it has shown increased hydroscopic qualities.
c) Estrogen Effect on Skin Wrinkling
Wrinkles show an alteration of dermal collagen, elastic fibers and marked decrease in glycosaminoglycans. Application of estrogen creams showed a marked improvement in fine wrinkles. Postmenopausal women using estrogen were less likely to develop skin wrinkles. Estrogen also causes increase in collagen and glycosaminoglycans in the dermis, which may explain the decrease in skin wrinkling with estrogen treatment. Treatment with estriol ointments to the skin showed changes in skin elastic fibers.
d) Estrogen Effects on Hair Growth
Hair growth encompasses 3 stages which are known to be influenced by estrogens. These stages are
- Growing or Anagen Stage
- Structural regression or Catagen Stage
- Resting or Telogen Stage
High estrogen levels (during pregnancy) prolongs the growing phase of hair follicle and low estrogen levels (post partum) result in significant hair loss (as anagen phase enters the telogen phase simultaneously), called androgenetic alopecia or female pattern hair loss observed after menopause. Estrogen treatment has shown increased anagen and decreased telogen as compared to placebo.
MECHANISM OF ESTROGEN EFFECT IN SKIN
Estrogens regulate cell function by binding to two nuclear receptors ER‐α and ER‐β. Mechanism of estrogen action on skin is not well known. There are controversies regarding expression of ER‐α and ER‐β. ER‐α and ER‐β are members of nuclear hormone family of intracellular receptors which is activated by hormone 17‐β‐estradiol. Function of estrogen receptor is as a DNA binding transcription factor which regulates gene expression. There are two receptors α and β, each encoded by a separate gene (ESR1 and ESR2). Hormone activated estrogen receptors form dimmers ER‐α (αα) and ER‐β (ββ) or homodimer ER‐αβ (αβ). While one group of researchers found that ER‐β is predominant receptor of skin, others found that both receptors are equally present in the skin.
ESTROGEN THERAPY FOR THE SKIN
1) Hormone Replacement Therapy (HRT)‐
Hormone Replacement Therapy or HRT consists of two components i.e., Estrogens and Progestogens. Use of estrogen alone is associated with an increased risk of endometrial hyperplasia. Thus progestogens are incorporated in HRT to protect the endometrium. As the estrogen component, natural 17‐β‐estradiol is often used in Europe, whereas the conjugated equine estrogen (CEE) derived from pregnant mare’s urine is the preferred product in the US. HRT carries a small increased risk of serious complications, and the risk increases with duration of the therapy. Recently, recognized experts have provided practical guidelines for postmenopausal HRT and have reviewed the risk of complications. Endometrial cancer occurs up to 4 times more frequently in women with a uterus who take unopposed estrogen than in non‐users. The risk may be reduced by adding progestogens. Breast cancer risk increases slightly with HRT prescribed longer than 5 years. Venous thromboembolism is rare but increases with estrogen use.
The indication for HRT is the treatment of menopausal symptoms (hot flushes, sweating, insomnia, fatigue, depressed mood and urogenital atrophy). The dose and regimen of HRT need to be individualized, based on choosing the lowest appropriate dose in relation to the severity of symptoms and on the menopausal age. Lower dose HRT has been shown to be effective and minimizes the side effects. Usually after 3‐4 years of hormonal treatment, it is possible to stop HRT with no recurrence of menopausal symptoms. Currently, experts believe that limited, shortterm use of HRT (<5 years) administered in the early phase of menopause is relatively safe among healthy women. Long term HRT may be appropriate if symptoms persist. In this case, appropriate counseling on the risks and benefits of the long term HRT should be provided. HRT can offer long term benefits in the CNS, CVS, and skeletal systems. Specifically, it has been demonstrated that HRT is very effective at preventing osteoporosis. However, there are still controversies about the long term use of HRT because of the risk of breast cancer with prolonged use of estrogens. In patients at high risk of osteoporosis, prevention should be continued independently of management of menopausal symptoms, using alternatives to HRT such as selective estrogen receptor modulators (SERMs).
Beneficial effects of HRT on skin ageing have been documented by several studies. An analysis showed that HRT prevents dry skin and wrinkling. Women under long term substitution had one‐third fewer wrinkles than non‐substituted patients. In a pilot study involving different regimens of HRT on skin ageing, patients were assigned into three groups based on their regimens:
a) Transdermal estrogen and progesterone
b) Transdermal estrogen
c) Oral estrogen and progesterone
And one group was kept as a control. Epidermal moisture, skin elasticity, and skin thickness were significantly improved in all treated groups. A comparison of epidermal hydration and skin elasticity revealed no significant differences between UV exposed and nonexposed measurement sites, suggesting that both intrinsic and photoageing may be improved by HRT.
A leading parameter of skin ageing is skin thickness, which reflects the status of collagen tissue. As previously reviewed, many studies have demonstrated beneficial effects of HRT on skin collagen content. HRT also affects skin elasticity; it has been reported that HRT also limits age‐related increase in cutaneous extensibility, thereby exerting a preventive effect on skin slackness.
Despite such beneficial effects of HRT on skin ageing, HRT cannot obviously be recommended solely to treat skin ageing in menopausal women. Prevention of skin ageing with HRT should be regarded as an additional benefit for menopausal women who receive this treatment for other menopausal symptoms.
2) Topical Estrogen Treatment-
Studies have showed that topical estrogen may prevent skin ageing, as seen with HRT. It was observed that treatment with topical 0.01% estradiol and 0.3% estriol on skin aging on the face of perimenopausal women for a period of 6‐months showed significant improvement similar to that seen in studies using HRT. Both treatments showed increased skin moisture and improvement of elasticity and firmness of the skin with decreased wrinkle depth. No hormonal side effects were noted, either clinically or by hormone monitoring. Serum hormone levels and the appearance of vaginal smears showed no significant change as compared to before treatment.
A group of scientists (Creidi et. al) examined the effect of a topically applied conjugated estrogen cream (Premarin) in 54 women. After a 24‐ week treatment period, they found that Premarin cream produced better results than the placebo cream; the difference was statistically significant for skin thickness and fine wrinkles. Premarin cream was well tolerated locally. The general safety of Premarin cream was also excellent; no women had any serious drugrelated study events. However, in contrast to the previous study, a modification of the vaginal maturation index was seen in women using Premarin cream, demonstrating that the CEE (Conjugated Equine Estrogen) has permeated the skin and exerted its effect on the vaginal mucosa. Indeed, it is known that CEE and 17‐ β‐estradiol differ in their total estrogenic potency. This suggests that estradiol creams may provide a safer therapy for skin ageing compared to CEE creams, since they seem not to induce systemic effects.
It is clear that topical estrogen is effective treatment for skin ageing. Menopausal women who are not receiving HRT and who do not have any contraindications to HRT would be candidates for topical estrogen therapy.
Since studies have demonstrated a sharp decline in skin thickness and collagen in the years following menopause, particularly in the initial postmenopausal years, it would be critical to begin the treatment within the first postmenopausal years. Additional studies are needed to definitively demonstrate the safety of this treatment. Further investigations should determinate the highest effective concentration of estrogens that can be used without the risk of possible systemic side‐effects.
Based on previous work on the use of topical estrogen forvaginal atrophy in postmenopausal women, it is expected that short term use of topical estrogen (<5 years) should prevent skin ageing without serious risks. Indeed, recent studies have demonstrated the efficacy and safety of a low dose of 17‐β‐estradiol for postmenopausal vaginal atrophy. Neither an increase in systemic estradiol, nor any estrogenic side effects (such as endometrial hyperplasia) have been observed with this treatment.
The choice of the form of estrogen is also important: as previously discussed, CEE, which possesses a greater estrogenic potency than 17‐ β‐estradiol, may induce systemic side effects. Estriol, a low potency estrogen that has considerably lower affinity for the estrogen receptor, is commonly prescribed in Europe for topical treatment of menopausal urogenital symptoms. This treatment has been demonstrated to be safe, with no increase risk of endometrial hyperplasia and so may be useful for topical treatment of skin ageing.
Such topical estrogen treatment for skin ageing will need to be administered by dermatologist experienced in endocrinology, given that the concentration and application areas must be observed in order to avoid systemic side effects.
3) Selective Estrogen Receptor Modulators (SERMs)
SERMs act at the level of the estrogen receptors; they bind to ER‐ α and ER‐β. They appear to have either estrogenic or antiestrogenic effects, depending on the tissue. In some tissues such as bone, they mimic the effects of estrogen, while in others they act as antiestrogens and block unwanted estrogenic effects on uterine and breast tissues. Because of this tissue specificity activity, SERMs are potentially a versatile drug class that offers the prospect of developing individualized, targeted treatments for menopause‐associated morbidity. SERMs and estrogen agonist molecules that are currently available or in development are shown in the table 2 below.
The question of whether estrogen alternatives such as phytoestrogens and SERMs are effective estrogens for the prevention of skin aging in postmenopausal women remains unanswered. However, preliminary data indicate that such treatment may be of benefit for skin aging treatment.
Effect of phytoestrogenic SERMs on skin ageing
Phytoestrogens are plant‐derived molecules that structurally resemble endogenous estrogens, containing a diphenolic chemical structure that can directly bind to estrogen receptor. They have a relative greater affinity for ER‐β than for ER‐ α. Phytoestrogens exhibit some estrogen agonist‐like properties but can also act as partial estrogen receptor antagonists. Because of their mixed agonist/antagonist estrogen receptor profile, phytoestrogens have received considerable attention as potential alternatives to estrogen. Studies have demonstrated that genistein may prevent photoageing in human skin. Other studies have reported that genistein and daidzein stimulate hyaluronic acid production in human keratinocyte culture. A recent European study had examined the effect of a cosmetic cream preparation including isoflavone (Novadiol) in 234 postmenopausal women and had showed improvement in the skin dryness and wrinkles after 12 weeks of treatment.
Effect of SERMs on skin ageing
An effective SERM for the skin would exert estrogen agonist action in skin and estrogen antagonist action in the breast and uterus. The ideal SERM for skin would also exert estrogen action in brain, bone and in the vagina. Among different SERMs currently available or under development, only raloxifene has been studied for its effects in skin. Raloxifene is used in prevention and treatment of postmenopausal osteoporosis. It also decreases the risk of breast cancer and does not stimulate the endometrium. Recent studies have demonstrated that raloxifene exerts stronger stimulative effects on collagen biosynthesis than estradiol in human skin fibroblasts and might reverse some of the postmenopausal changes in skin.

- Figure 1 – Shows a list of SERMs and Phytoestrogens that are available or in development

TO SUMMARIZE ESTROGEN TREATMENTS
The skin is an estrogen responsive tissue. A better understanding of the hormonal regulation of skin physiology and skin ageing may provide the basis for development of new hormonal treatment for skin ageing. HRT cannot be recommended solely to treat skin ageing in menopausal women but may be considered as an additional benefit in the treatment of menopausal symptoms. Topical estrogen application is highly effective and safe if used by a dermatologist with an expertise in endocrinology. Phytoestrogens appear to be effective but their possible side‐effects have not been well investigated. SERMs are drugs that offer exciting opportunities for the future treatment of skin ageing but, while great strides have been made in developing effective SERMs for menopausal symptoms such as osteoporosis, the challenge of developing an effective estrogen alternative for skin ageing treatment remains.
References
- Elderly skin and its rejuvenation: products and procedures for the aging skin, Marcia Ramos‐e‐Silva et. al., Journal of Cosmetic Dermatology, 6, 40–50
- Effect of estrogens on skin aging and the potential role of selective estrogen receptor modulators. S Verdier‐Sévrain Climacteric; Aug 2007; 10, 4; Health Module pg. 289