The four processes involved when a drug is taken are absorption, distribution, metabolism and elimination or excretion (ADME).
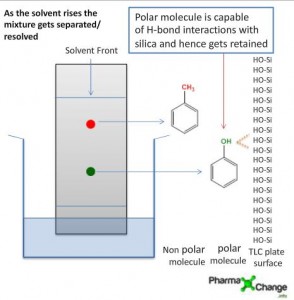
Pharmacokinetics is the way the body acts on the drug once it is administered. It is the measure of the rate (kinetics) of absorption, distribution, metabolism and excretion (ADME). All the four processes involve drug movement across the membranes. To be able to cross the membranes it is necessary that the drugs should be able dissolve directly into the lipid bilayer of the membrane; hence lipid soluble drugs cross directly whereas drugs that are polar do not.
. Taken from reference 3.")
Absorption
Absorption is the movement of a drug from its site of administration into the blood. Most drugs are absorbed by passive absorption but some drugs need carrier mediated transport. Small molecules diffuse more rapidly than large molecules. Lipid soluble non – ionized drugs are absorbed faster. Absorption is affected by blood flow, pain stress etc.
Acidic drugs such as asprin will be better absorbed in the stomach whereas basic drug ike morphine will be absorbed better in the intestine. Most of the absorption of the drug takes place in the small intestine. Since the surface area of the stomach is much smaller than that of the intestine. Most of the drugs are absorbed in the small intestine since the amount of time that the drugs spend in the stomach is less and also the surface area of the stomach is small. If a basic drug is taken after a meal then the activity of the drug can be reduced whereas if an acidic drug is taken after a meal then the action of the can be noticed much more quickly, owing to the gastric absorption.
For a drug even though lipophilic to be absorbed in the intestine some portion of it needs to be dissolved in the intestinal juices which are aqueous. There are some substances that are partly soluble in water and it is these that will be absorbed and then an equivalent amount will be absorbed from the undissolved portion. Thus complete absorption will take place. There are bile salts present in the intestine which will aid in salvation of the drug and their resultant absorption. Drugs that are amphipathic have no problem in getting absorbed. There are some drugs that are completely insoluble in water such drugs float as globules in the intestine but the bile salts will emulsify these into small enough particles such that absorption can take place. E.g. vitamins. Some of the drugs are similar to compounds found in the body for e.g. thyroxine and such drugs can be absorbed into the system by active transport.
When drugs are injected into the muscle, subcutaneous layer absorption still has to take place but it is less dependent on the chemical nature of the drugs since the drugs are absorbed into the circulatory system through the small pores in the capillary walls.
Distribution
Distribution is the movement of drugs throughout the body. Determined by the blood flow to the tissues, it is ability of the drug to enter the vasculature system and the ability of the drug to enter the cell if required.
Plasma Protein Binding
The blood stream has the ability to transport relatively insoluble substances. These substances are transferred by binding to the proteins which have a very amphipathic structure. The hydrophilic group renders the protein soluble in water and the lipophilic compounds are attracted to the lipophilic group and are loosely bound to the protein molecule hence protein bound. Most of the drugs travel in the plasma are partly in solution and partly bound to the plasma protein. The bound drug is inactive and the unbound drug is active. The ratio of bound to the unbound drug varies. Binding is reversible. Generally acidic drugs bind to albumin and basic drugs to α1 – acid glycoprotein. Diseased state can cause a problem on the effectiveness of the drug. As globin levels increase with age this factor should be taken into account when treating an elderly person with a basic drug.
The protein bound drug is in equilibrium with the free drug. That means that once the free drug enters the target tissue then the protein bound drug will be released to maintain equilibrium. If two drugs bind at the same site of the protein and are administered together then there can be problems. e.g. Warfarin and asprin.. asprin displaces warfarin from its bound protein as a result of which there are elevated levels of warfarin in the unbound state and this can lead to warfarin toxicity.
Tissue Distribution
After absorption most drugs are distributed in the blood to the body tissue where they have their effect. The degree to which the drug is likely to accumulate in the tissue is dependent on the lipophilicity and local blood flow to the tissue. Highly perfused organs receive most of the drugs.
The role of the liver in drug distribution
After the drug is absorbed by the GI tract, it is taken up by the part of the bloodstream called the hepatic portal system. Most of the drugs are absorbed into this system except for the lipids which are absorbed into the lymphatic system and then delivered into the blood by the thoracic duct into the superior vena cava.
The hepatic portal system is designed to take digested foodstuff into the liver where it can be processed, in some cases it is stored before being distributed and it is possible that this may happen to the drug and the drug would be metabolized before reaching the rest of the body. Such drugs that metabolized by the liver are said to have a high hepatic first pass. Hence drugs with a very high hepatic first pass cannot be given orally.
The Blood–Brain Barrier (BBB)
The capillaries in the CNS are different they have pores which are sealed by the connective tissue and hence only small molecules can cross the blood brain barrier and the substances that can cross over have to be very lipophilic in nature. The blood-brain barrier (BBB) is the protective mechanism of the CNS and is not present everywhere in the brain. This is sometimes useful as it avoids some drugs from crossing the CNS and causing deleterious effects. E.g. neuromuscular blocking agents. Sometimes the blood brain barrier allows the transport of drugs resulting in unwanted effect for e.g. antihistamines cross the bbb and result in drowsiness, now there are antihistamines that are made that are not so lipophilic in nature.
Metabolism or Biotransformation
It is the process of transformation of a drug within the body to make it more hydrophilic so that it can be excreted out from the body by the kidneys. This needs to be done since drugs and chemicals are foreign substances in our body. If the drug continues to be in the lipohilic state and is going to be filtered by the glomerulus then it will be reabsorbed and remain in the body for prolonged periods. Hence metabolism deals with making the drug more hydrophilic such that it can be excreted out from the body. In some cases the metabolites can be more active than the drug itself e.g. anxiolytic benzodiazepines.
Some enzymes are highly specific and will breakdown only compounds that they recognize for e.g. glucose dehydrogenase. But there are some enzymes such as pepsin which are not specific and will breakdown most soluble proteins into smaller polypeptides or amino acids. This enzyme and many other proteolytic enzymes attack the peptide bond that joins the amino acids to make proteins, and in this way break the protein down.
Two types of enzymes are involved in metabolism:
Phase I Metabolism
These enzymes modify the drug chemically by processes such as oxidation, reduction and hydrolysis or by the removal and addition of an active group.
Phase II Metabolism
These include the conjugation of a drug or a phase I metabolite with a polar group to render it possible for excretion. e.g. sulphates and glucuronide
The deconjugation of the drug by bacterial enzymes is called the enterohepatic cycle. Sometimes this deconjugation can lead to increased levels of drugs in the body. But some times due to treatment with antibiotics there may be less or no deconjugation as a result of which there will be less drug in the body.
Principal sites of metabolism are Liver and Kidney and once the drug is rendered hydrophilic they can be easily excreted out by the bile and urine without significant reabsorption.
Enzyme Induction
There are some drugs that can lead to an increase in the production of the enzyme and as a result speed up the metabolism of the drug and hence a higher dose of the drug is required to achieve the therapeutic effect.
Enzyme Inhibition
Some drugs result in the inhibition of certain enzymes and as a result there is an accumulation of the drug in the body and can lead to drug toxicity. This is also a form of drug – drug interaction.
Excretion
Excretion is the removal of the substance from the body. Some drugs are either excreted out unchanged or some are excreted out as metabolites in urine or bile. Drugs may also leave the body by natural routes such as tears, sweat, breath and saliva. Patients with kidney or liver problem can have elevated levels of drug in the system and it may be necessary to monitor the dose of the drug appropriately since a high dose in the blood can lead to drug toxicity.
Drug Dosage and Drug levels – Basic Definitions
Half life of a drug is the time for the drug to decrease to half of its concentration.
Minimum effective concentration: below which there will be no therapeutic effect.
Maximum safe concentration: above which there will be a toxic effect The larger the therapeutic index the more safer the drug.
Bioavailability: It describes the amount of drug that is available to the body to produce a therapeutic effect.
Onset of action : it is the time taken for the drug to reach the minimum effective concentration after a drug has been administered.
Peak Action: occurs when the drug reaches its highest blood or plasma concentration
Duration of action: is the length of time the drug has a pharmacological action.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics by. Joel Griffith Hardman, Lee E. Limbird, Alfred G. Gilman. 10th Ed.
- Rang & Dale’s Pharmacology by. Humphrey Rang, Maureen Dale, James Ritter, Rod Flower. 6th Ed.
- PK/DB – Database for Pharmacokinetic Properties – IFSC/USP (URL= http://miro.ifsc.usp.br/pkdb/) accessed – April 09, 2011.
Wow! This page is very helpful, I’m a college student and it did give me some information to do my assignment. Thank you very much.
Thanks well understood
This website was… how do I say it? Relevant!! Finally I’ve
found something that helped me. Appreciate it!
Nice material,kodus to your write up.
. helpful indeed. easy enough to understand. thanx. 🙂
Very helpful info… thanks
having had addisons disease for 33 years, having led a normal life wo any addisons problems which require stress dosing, or hospital stays, i now find myself unable to work or do much of any activity. all these years ive been on 25 mg cortisone acetate and .1 mg fludrocortisone in the am. 12.5 mg cortisone acetate in the pm. since march of 2013 the last company to make this drug stopped production, wo notice.my endo tried 5 different types of steriods over a 6 month period, but nothing would allow me to get out of bed, after researching the availabilty thru out the world, i found it in canada, but having been on it for 7 months , my activity is limited to 15/20 min at a time w several hours rest before the next activity. my blood tests r normal, main organs r fine,my question is what process is limiting absorbtion in my muscles, hence the extreme fatige , im in no pain all seems normal. what source am i looking for to answer these questions, why r blood tests normal, why no problems w main organs except for all muscles, whats happening that muscles r ok but only for this extreme short periods,and the muscle activity does not return at the same level. i have been looking into pharmacokinetics as a possible lead to the next solution. all leads will be studied, ty for your time.if age means anything im 55
Pharmacokinetics – I was expecting to find things like half-life
how can you talk about this topic and not use that term?
We will be putting up more articles in the future with half-life and equations of orders of absorption. But this is the basics of pharmacokinetics beginning with ADME.
this page makes realise the truth in pharmacy
this page is very helpful…….thanx……..
Thanks